
CT testing for COVID: Benefits exceed risks
Cite as:
Chen Shen, Jenifer Siegelman, and Yaneer Bar-Yam, CT testing for COVID: Benefits exceed risks, New England Complex Systems Institute (June 11, 2020).
We estimate the benefits from the use of CT scans in conjunction with RT-PCR for diagnosis of COVID- 19 in symptomatic individuals. Our calculation shows that for 10,000 CT-scans 124 lives are saved this year (within months), 2,074 diagnosed cases are prevented, 415 hospitalizations are prevented along with subsequent short and long term disability. Well established estimates imply 1 future cancer may result.
The use of CT scans in conjunction with RT-PCR for diagnosis of COVID-19 in symptomatic individuals can address the problems caused by 30% false negative rate RT-PCR, time delays in obtaining results, and limited availability [1]. The high false negative rate means almost 1 in 3 infected individuals with mild symptoms are informed they are not infected and will not isolate and thus infect others. Moreover, since effective isolation is difficult, symptomatic individuals do not completely isolate after testing while pending results. Given the extended turnaround time for diagnostic PCR results, individuals with COVID-19 continue to expose others to the virus. Using CT scans with immediate interpretation by radiologists (or in the future AI algorithms) reduces the time an infected individual can infect others, low false negative rates further contribute to the reduction in transmission.
Here we analyze the benefits obtained in an outbreak context for CT screening of symptomatic individuals. Our results show that for 10,000 CT-scans 124 lives are saved this year (within months), 2,074 diagnosed cases are prevented (out of a total of 3,039 cases), 415 hospitalizations are prevented, along with all of the subsequent short and long term disability that will impact health, healthcare costs and society as a whole in the upcoming years. The outbreak duration will be shortened enabling economic activity to be restored. An often expressed concern is the potential for CT-scans to cause cancers. We calculated the expected cancers resulting from the CT-scans. Screening of symptomatic individuals can be performed with low dose non-contrast CT-scans (LDCT are currently reimbursed by governmental payers in the US at roughly $70-130 by Medicaid and Medicare respectively). The low level of radiation exposure from LDCT has not been shown to cause cancer. However, the currently accepted model of predicting lifetime risk of fatal cancer is 5% per sV given to a population [6]. This estimate implies 1 fatal cancer per 10,000 patients scanned using a 2 mSv LDCT [2].
The number of COVID cases prevented by use of CT-scans can be calculated from the reduction in effective reproduction rate R given by ∆ = 0.2 [1] and written as:

where M is the number of scans performed, q is the fraction of positive test results (Mq is the number of infected individuals scanned) and R_P is the reproduction ratio for widespread use of PCR testing.
We note that if the outbreak is growing, R_P ≥ 1 this is infinite, i.e. stopping the down stream cascade of each case results in a large number of cases limited only by the population size. It is finite if the outbreak is declining R_P < 1. We estimate the benefits starting from a decreasing outbreak with a value determined by recent rates of decline in Massachusetts and New York (Appendix). For Massachusetts and New York at the current time R_P ≈ 0.86. Other cases can be similarly estimated. Taking q = 0.05 which is appropriate for widespread testing [3-5] we have:

Thus the number of cases prevented is 2,074 (out of a total of 3,039 cases), and for estimated rates of hospitalizations and deaths for symptomatic cases determined by widespread testing of 20% and 6%, we have 415 hospitalizations and 124 deaths.
For a sensitivity analysis we can perform the same analysis for a more rapid decline in rate of cases in NY where R_P = 0.77 for which we would prevent 1,037 cases (out of a total of 1,710 cases), 207 hospitalizations and 62 deaths within weeks of performing the CT-scans.
We estimate the additional incidence of cancer from the established result for Low Dose CT of an incidence of .05% cases for every 1000 mSv [6]. For 10,000 Low Dose CT (2 mSv) scans this gives 1 fatal cancer.
Every potential COVID patient who is prevented from infection reduces costs not only for immediate hospitalizations but also for long term sequela associated disability which will have a measurable cost in the upcoming years. Primary prevention results in zero downstream costs for all those patients.
We note that in our analysis, since the prevention is of cases that will be infected, the age of the individual being tested by CT does not affect the benefit in decreased disease, death and disability. Also while the existence of undiagnosed individuals including asymptomatic ones is not well characterized, our analysis counts known infections in relation to observed transmission so we have not included prevention of undiagnosed or asymptomatic individuals. Thus, the uncertainty in their proportion does not affect this analysis of benefits.
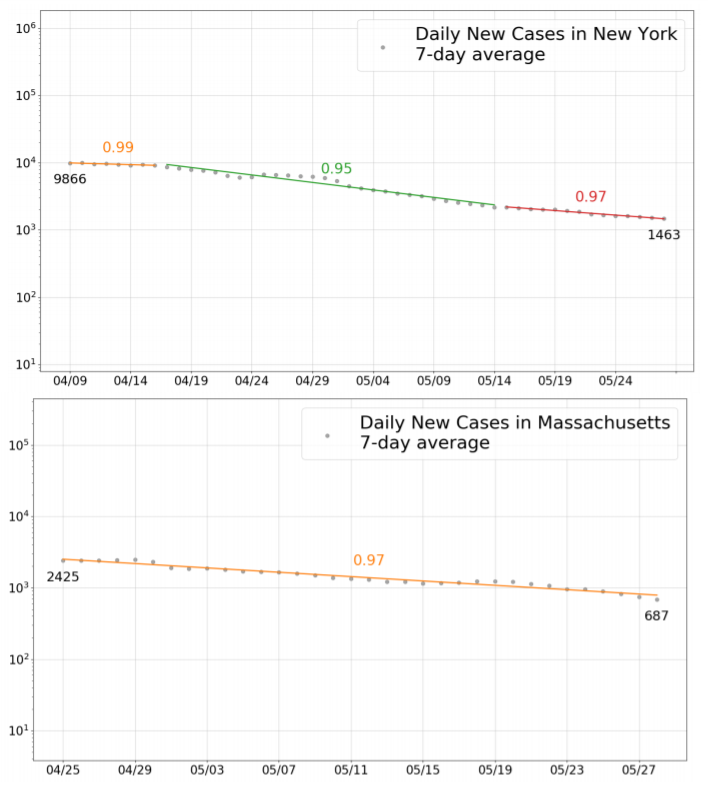
Fig. 1. Rates of decline of outbreak measured in daily multiplier for New York (top) and Massachusetts (bottom).
I. Appendix
We determine the value of R_P = G^τ for Massachusetts and New York (See Figs. 1 and 2), with G the daily multiplier of new cases at this time of G = 0.97. The typical infection time is τ = 5 days, so we obtain R_P = 0.86. Earlier in New York the daily multiplier G = 0.97 would have given R_P = 0.77.